Índex
CURRENT SITUATION OF GERIATRIC RESIDENCES
Everyone wants to age at home, so that the residenciesshould be so, as the home of each of their residents. Instead, what we have today are residencies where elderlypeople are clean and nursed, where they care about shifts,management and security, with clean, impersonal,institutional and safe spaces. It is proven that there is a direct relationship betweenarchitectural design and subjective wellbeing. The creationof positive environments is, together with the attention ofpeople, one of the pillars of the AICP model. To achieve spaces that promote the autonomy andindependence of people, which promote social relations andpertinence to a group, but which also protect intimacy andindividuality must be objective in the design of theresidence, a Architecture conceived from the user and by theuser, an architecture conceived by the person. The residencies are not hospitals or hotels, they must behomes for their residents. Historically, the residencies have evolved from thesanatorium and hospital model; Concepts such as beds as aunit of measurement or control areas of nursing have beenthe residencies themselves. Historically, the residencies have evolved from thesanatorium and hospital model; Concepts such as beds as aunit of measurement or control areas of nursing have beenthe residencies themselves Traditional centres and services are based on an idea and anorganization of care where people’s autonomy is seriouslyrestricted. The existence of rules derived from the purelyorganizational objectives, the limited flexibility in attention,more focused on the realization of scheduled tasks thanwhen caring for people, reduce the capacity of residents totake their Own decisions and exercise control over their dailylives. The architecture of these residencies has been impersonal,where functionality, hygiene and regulatory compliance areprioritized, above generating environments that promotethe welfare of residents. The spaces of food or are where the residents are, tofacilitate the control and management, have been spacesthat generated stress and discomfort to the users.
THE PHYSICAL SPACES OF RESIDENCIES BASED ON THE AICP MODEL
The architectonic structure of the rates based on the ACP model has to be arranged in units of coexistence, 14 to 16 people, combining private spaces and shared spaces. It consists of a common space that includes a kitchen, dining room, lounge and an excess of an outer space.
The lifestyle of the living units is similar to that of domestic environments, both in environment and in routines, schedules and activities.
Prioritising the principles that govern the model of AICP (autonomy, integrity, individuality, social integration, independence and continuity of care), the keys to design in these residencies have been:
-Location of the center in an urban environment: is part of the memory of the residents, guaranteeing the continuity with the previous life and the maintenance of social relations.
-Outdoor landscape considered as a therapeutic environment. The view of the exterior is a fundamental rule of design, to facilitate the presence of light, which favours the spatial-temporal orientation. The natural outdoor spaces (gardens, terraces…) favour the active life of residents, their independence in safe and controlled environments.
-Universal design criteria understood as the design of an environment, building or product that can be used and understood for the whole world regardless of its age, size, ability or disability.
Ensure easy and full accessibility to all spaces, guaranteeing the independence and security of all users.
Establish designs and strategies that facilitate the orientation of the users, so that at all times you can find, identify and use the different places and spaces without asking for help.
–Stimulation of social interaction. Designing spaces that favour meetings and communication between people, as well as socialization and permanence in the social groups of residents.
-Promotion of independence. Residents have the right to privacy and privacy, for those who are projecting units with a maximum number of single rooms.
-Stimulation of the senses. Special care has been taken with the acoustic comfort, the ventilation and the renewal of the air to avoid odors, the hygrothermal control of the different spaces, maximum natural light in all spaces with solar control of the windows and French balconies
-Promote the natural illumination of all the spaces, since the natural light has incidence in the cycle of natural light has incidence in the rhythm circadian and in the orientation spacetemporal of the residents.
-Take care of the quality of the interior air and the ventilation, since they play a decisive role in the control of the concentrations of pathogenic agents; It is to combine natural ventilation systems with mechanics to take advantage of the climatologic qualities of the area and amortize the energy consumption of the building.
-Creation of affective and safe environments, by the presence of the plants and participating residents in the decoration of the spaces.
It is important to use the culturally relevant and familiar materials for users, who at the same time are compatible with sanitation, maintenance and functional requirements.
-Single rooms, to preserve the intimacy and independence of residents, as well as rooms that can be personalized to create continuity with the previous life, allowing residents to bring their own furniture, photographs and Decorative objects.
-Co-design, using architecture as a design strategy that promotes participation in the decision-making that concern the end user (personalizing the spaces, establishing participatory strategies for users who require the Coordination between design and management teams, training of working groups with residents).
The goal is to achieve spaces where residents feel their home where to develop a life project.
CASE STUDIES
THE ADECUATION OF THE RESIDENCIA DE SANT HILARI SACALM
The residence of SANT HILARI SACALM is the ADECUACIÓN of a residence of 54 users, in full activity, to the model AICP. The project consists of changing the traditional functional structure of the centre and creating independent cohabitation units.
The building has 3 floors and takes advantage of the topography of the plot to have direct access to the exterior in each one of them. The location in an upper area of the municipality makes the residence incorporate the landscape as part of the decoration.

Part of the residence, integrated in the surrounding area and the privileged natural landscape.
Before the adaptation, the residence was structured givingthe service to 30 residents grouped in double and singlerooms. The sleeping areas are located on the floors and thecommon spaces (dining room, living room..) are located in asingle space on the ground floor. This situation causes oftencommon spaces to be insufficient for the accumulation ofresidents in the hours of influx. In addition, a very controlledand impersonal environment was generated because ofhaving a high number of people in the room without beingable to be dealt with personal form.
As a result, users spent most of the time in the rooms,without having to relate to other colleagues and withoutenjoying the outer space.
PROJECT
The project to adapt the AICP-model residence is based onthe desire to offer the best service to the residents and,ultimately, to improve their physical and mental WELLBEING.Therefore, it aims to promote the PARTICIPATION of users,making them partakers of the life of their community and atthe same time, offering an environment closer to theirprevious life.
The unity of coexistence has an irregular geometry that hasbeen used to organise it in two environments (dining roomand living area) articulated by an open kitchen, in the interiorarea. In month the space has a direct access to an outdoorterrace with views of the municipality and the landscape.
The dining area is organized by grouping tables so thatdifferent configurations can be achieved according to theneeds of each moment. The FLEXIBILITY of the space hasbeen an important premise, so that the design of theelements, so much of the installation of lighting, heating orfurniture not interfere with this objective.
The living area is also organized in environments such as theTV area, an electric fireplace and a library area, so wegenerate SOCIABILIZATION spaces but also individual placesto be contempled.

Articulating these spaces is located the kitchen, with mobile boards in height, which facilitate the participation of residents in everyday events as are the preparation of the breakfasts or even the washing of the crockery

The principle of independence and autonomous living of residents, cooking or planing their clothes.
They also have a washing machine and a ironing area that encourages the AUTONOMY and PLANNING of residents in domestic routines that have made in the long run of their lives.
At the time, the space available had different levels that were saved with secluded stairs, next drawback to people with reduced mobility. Based on a principle of ACESIBILITY and INTEGRATION the main performance was leveling the entire space moving the gap to access through a slight ramp, guaranteeing mobility for all users.

It is a space that encourages the sociabilization of residents and active life
According to the AICP model, several meetings were held during the work with the residents, accompanied by their relatives and the staff of the Centre, to participate actively in the interior design of the space. In the end, Ham was themselves who have decided the colours of the walls, the choice and even the furniture.

During the work, several design options have been presented so that the users decide which was the best solution.
CHANGE OLD HOSPITAL OF OLOT
The project of the RESIDENCIA SANT JAUME D’olot consists of the TRANSFORMATION of the former hospital of Olot into a residence as a model of comprehensive care centred on the person (AICP) of 64 residents, organized into 4 independent cohabitation units.
It is a building with an extensive history in the town of Olot, since it was built in the 16TH century and today it is considered a CULTURAL LOCAL (BCIL). During the SIXTEENTH century, a private initiative promoted the transfer and construction of a new hospital that would be located where it is currently, a key point of high personal flow and slightly separated from the new urban fabric that is developed around the main square.
The hospital has been in operation until 2000 a strategic plan was developed confirming the lack of space for the different services of the center and the need to build a new hospital, leaving this building as a geriatric residence.
Project
Today the geriatric residence service of 64 residents. The state of conservation of the building requires a reform to update and adapt the space to the current needs, and this is why the project consists in the TRANSFORMATION of the building with the model AICP.

Images of the current state. The residence requires a transformation to adapt it to the current needs.
For the development of the project, the historical relevance of the building has been taken into account, both architectonic and historical point of interest of the municipality.
A criterion that sustains the AICP model is the importance of the ENVIRONMENT where the centre is located. In this case, without doubt, we are in a privileged environment, in the heart of the old town of Olot and in a historic building. This situation favours the well-being of users, who are in a well-known place, which is part of their memory, guaranteeing the continuity of their previous life and the maintenance of social relations.
To emphasize this nature of permanence of the home, the main access of the building is relocated in the historic courtyard, so that the centre appropriates it and incorporates it as a space of activities.

New access from the central courtyard
The upper floors are organized from a perimeter corridor around the courtyard, which connects the entire floor and recovers the original circulation of the cloister. This way you get a CLEAR and UNDERSTANDABLE ORGANIZATIONAL scheme for any user.
The cohabitation units are distributed in one on the first floor and 3 in the second floor. On the first floor we find the general services of the residence of the north wing, and the unity of coexistence in the south wing taking advantage of the existing terrace. On the second floor, we find 3 units of cohabitation united by the central corridor around the courtyard. 1 unit is located in the north wing, the other to the west and the last in the south, as in the first floor.
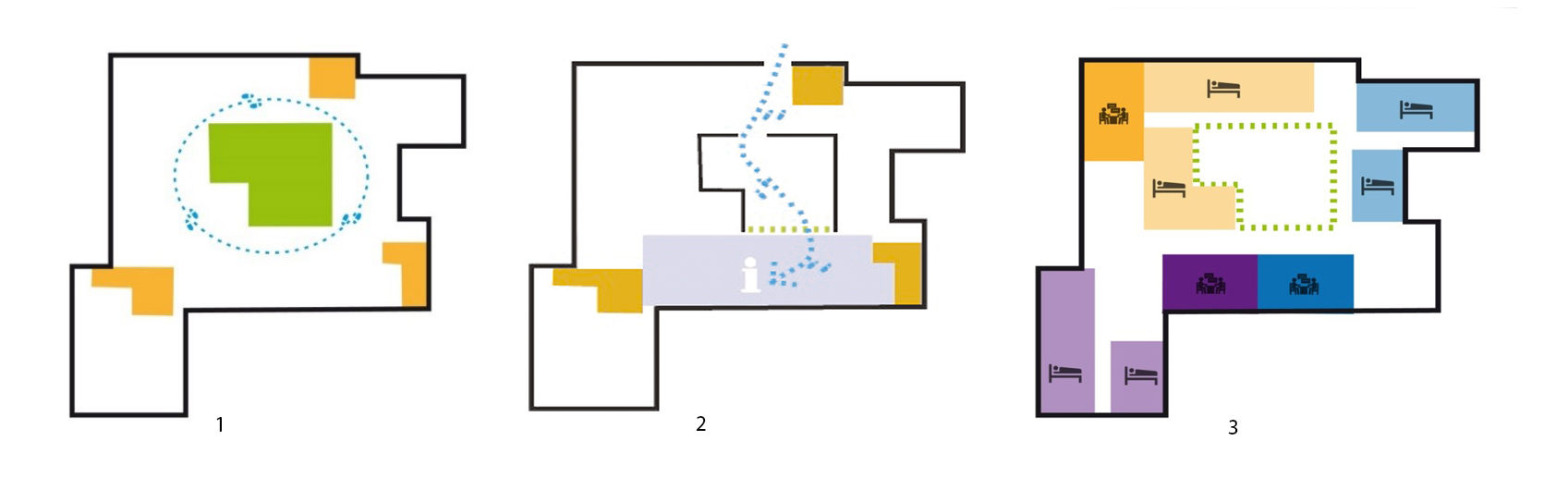
1. Organization around the courtyard to recover the original circulation of the cloister.
2. New access from the inner courtyard.
3. Distribution of coexistence units around the courtyard.
Each unity of coexistence is designed for a maximum of 16 residents, it is organized with double and single rooms to maintain a maximum number of users and guarantee the sensation of privacy and intimacy. It is also required to favor the autonomy of users at all times, offering diversity of resources, programs and services to minimize dependency situations and encourage people to display their preferences and choose between various Related to the worrying issues affecting them.
The rooms are the most intimate and personal point of the users. It is important that a space is offered with an AFFECTIVE and CALID ENVIRONMENT, where users feel at home. That is why it has been designed with very identifiable materials such as in the home, like the LVT pavement with appearance and wood texture. Even to involve users of these decisions, groups of work have been organized with patients to assign the rooms and that each can personalize the color of their room, as well as decorative elements.

The warm atmosphere of the materials used stimulates positive emotion. The decorative elements favour the succession of the positive knowledges.
Each unity of coexistence also has a living-dining room as a nerve point of SOCIAL INTERACTION. It is a space for people to interact with those in their surroundings, enjoy the company-both their colleagues and the staff-and have a space where they feel comfortable outside of their space but the room is. In addition, they have an adapted kitchen, as well as the adequacy of the spaces for the washing machine and the griddle to promote the INDEPENDENCIA and AUTONOMY, so that people can feel that they can develop their own plan of life, routine and make decisions in aspects Important of his life.

La residencia representa la cara amable i la calidesa humana de la arquitectura i el disseny. Ideat per crear records i emocions.
The unit creates 2 ambiences: Dining room, organized arounda kitchen, equipped with a mobile counter in height,microwave, refrigerator and sink. The living room is organizedon 2 sides, an electric chimney and library, and the other withsofas and TV.

With the TRANSFORMATION that the project has, it is achieved by considerably improving the lifestyle and comfort of the users. It moves from a model based on dependency, and generalization to a model focused on the individual user, where he can feel in a warm and safe environment where he heard that continues to have control of his own life and decision-making in everyday events.

